The association between talcum powder and increased risk for ovarian cancer and mesothelioma is one that simultaneously is the focus of much research and the object of extensive litigation. Industry leaders and researchers have spent a great deal of time and money bolstering their arguments concerning talc’s possible relationship to both ailments.
With that in mind, there is relatively little discussion elsewhere regarding some other potential illnesses associated with talcum powder products, as well as other possible cancer risks. Talc-based baby powder products can cause respiratory ailments for both babies and adults alike if inhaled. Additionally, some research has associated talc with other cancers such as lung cancer and uterine cancer.
Talc and Asbestos – A Key Distinction
Talc is a naturally occurring mineral that appears as almost grey or green with a greasy type of texture. When talc is processed, crushed, dried, and milled – it develops its signature soft, white powdery look and feel. Historically, talc has been mined in close proximity to concentrated asbestos deposits. Asbestos is a well-known carcinogen. Therefore, it has been understood for some time that naturally occurring talc will contain some amounts of asbestos.
Over the years, talc’s properties for moisture absorption and friction reduction have made it a very popular ingredient in many household items such as baby powder and a range of cosmetic products. However, concerns about asbestos exposure led the Cosmetics, Toiletry and Fragrance Association (CFTA) to develop an internal “self-policing” standard within the United States wherein members agreed that their products should be free of “detectable amounts” of asbestos. The World Health Organization (WHO) does not believe that any amount of asbestos is safe, detectable, or not.
Accordingly, when thinking about talc and the risk for cancer and other diseases – it must be remembered that some manufacturers claim that their talc products are “asbestos-free”. It is an important distinction because the linkage between cancer and asbestos is clear. The link between talc-free asbestos and the risk for illness is not as well understood or researched.
Talc Inhalation and Pneumonia Risk
Infants and children may suffer from “acute talc inhalation” symptoms, although the condition is very rare in adults. When applied to the skin, talc is largely harmless. However, talc does not dissolve in water and when inhaled immediately sets to dry up mucous membranes in the windpipe and lungs. Coughing or sneezing symptoms ranging up to sometimes fatal severe respiratory distress can result.
Infants and children suffering from acute talc inhalation must receive immediate medical attention. Treatment will usually involve medication to stimulate the bronchial passageways in the lungs and chest x-rays to monitor for inflammation as well as the administration of antibiotics to counter any possible onset of bacterial pneumonia.
Other Potential Cancer Risks from Talc
Stomach Cancers
A March 2019 article in the International Journal of Environmental Research and Public Health studied the potential for increased risk of stomach cancers from ingestion of asbestos-free talc. The study focused upon a population in Taiwan that had consumed Chinese herbal remedies that contained asbestos-free talc (commonly used as a diuretic and antacid). The study was conducted through Taiwan’s health insurance registry database and participants were followed to learn of any diagnosis of stomach cancer. At the conclusion of the study, researchers believed there is a “positive association” between increased stomach cancer risk and ingestion of asbestos-free talc.
Uterine and Cervical Cancers
Over the years, a range of studies and research have discovered a positive association between “dusting” of the female genitalia with talcum powder and an increased risk of ovarian cancer. The International Association for the Research of Cancer (IARC), a unit of the World Health Organization (WHO) classified “perineal use” of talcum powder as a “Group 2B” human carcinogen in 2006. Specifically, the IARC found that between 16-52% of women in the world used talcum powder on their genitals and that among them there was an increased risk of ovarian cancer ranging from 30-60%.
While there has been a great deal of credible research on the linkage between ovarian cancer and talcum powder, not as much attention has been focused on a possible relationship to other female reproductive ailments. A 2011 article in the journal Cancer, Epidemiology, Biomarkers, and Prevention reported on a study of over 66,000 women with nearly 600 cases of uterine cancer diagnosed between 1982 and 2004. The study suggested that there was an association between talcum powder and uterine cancer, particularly among postmenopausal women.
Other studies have found no linkage between talc and uterine or cervical cancers. The American Cancer Society and other experts agree, however, that further research is needed to explore the potential risk.
Lung Cancer
The risk of lung cancer from exposure to inhaled asbestos is well established. Asbestos is one of the most well-documented carcinogens known to the medical profession. However, the cancer risk from asbestos-free talc is less understood, outside of an industrial or mining setting. A 2006 study of talc miners and millers did not observe any higher rate of lung cancer mortality rates, outside of other risk factors such as smoking. However, other studies have suggested a possible link between long-term industrial exposure without drawing any specific conclusions. Experts agree though, that additional research is warranted.
As far back as the 1960s, medical researchers first suggested the possibility that talcum powder sprinkled on female genitalia could be linked with ovarian cancer. Their belief stemmed from the knowledge that talc naturally contains asbestos, a fibrous mineral with a well-established connection to increased cancer risk. Years later, in 1982, scientists conducted the first case-control study to link talcum powder and ovarian cancer. Since then, more and more studies have followed confirming an association with increased risk.
Talc is a naturally occurring mineral that can be crushed, dried, and milled to form a fine, soft, white powder that has a propensity to absorb moisture and reduce friction. Usually, talc is mined in close proximity to deposits of asbestos. Despite the potential for asbestos contamination, talc has been a very popular ingredient in personal care and cosmetic products in the United States for decades. In 1976, in an effort to beat federal and state regulators to the punch, an industry trade association, the Cosmetics, Toiletry and Fragrances Association (CTFA) proposed that the industry be allowed to self-regulate with voluntary standards requiring that all member companies market products which are “free of detectable amounts of asbestos”. “Detectable” is an important distinction as many research experts will contend that even small or virtually undetectable amounts of asbestos can potentially increase cancer risk substantially.
Products such as Johnson & Johnson Baby Powder were aggressively promoted to American consumers for over a century. Originally pitched as a drying and diaper friction solution to mothers for their babies, use of talcum based powder began to wane as parents, concerned with risks from inhalation, switched to other solutions such as corn starch. Accordingly, manufacturers of talcum powders began to switch their marketing focus toward women in general, promoting talcum powder as a solution for genital odors, perspiration, and moisture. Johnson & Johnson even specifically targeted “curvy” and overweight African-American women in its advertising as the use of baby powder underwent a demographic shift. These campaigns were wildly successful and by the mid-2000s, adults accounted for 91% of Johnson’s Baby Powder use.
Despite the studies and evolving knowledge concerning the association between talc-based powders and ovarian cancer, Johnson & Johnson and other manufacturers continue to insist that their talc-based powders are asbestos-free and do not cause cancer. And to be sure, there exists no definitive evidence that talcum powder causes ovarian cancer. Nevertheless, in May 2020, Johnson & Johnson announced that it was discontinuing sales of talc-based powder products in North America. The company will allow existing bottles of baby powder to be sold by retailers until supplies run out.
Evolving Understanding of Ovarian Cancer Risk
The first epidemiologic study involving talcum powder use on female genitalia was performed in 1982 by Dr. Daniel Cramer and his team of researchers. Dr. Cramer’s study found a significantly increased risk of ovarian cancer in women who reported that they regularly used talcum powder in their genital area. According to Dr. Cramer, officials from Johnson & Johnson came to discuss his study. At that time, Dr. Cramer recommended to Johnson & Johnson that they place a warning on its talcum powder about the risk of ovarian cancer. Since the Cramer study, there have been approximately 22 additional epidemiologic studies that have reported an elevated risk for ovarian cancer associated with talcum use on female genitalia. Among these studies and findings:
In 1993, the U.S. National Toxicology Program (USNTP) published a study on the toxicity of non-asbestiform talc and, according to their statement, found clear evidence of “carcinogenic activity”.
The International Association for the Research of Cancer (IARC), a unit of the World Health Organization (WHO) published a paper in 2006 wherein it classified perineal use (i.e. in the area of the female genitalia) of talcum based powder as a “Group 2B” human carcinogen. IARC is widely accepted as the international authority on cancer issues.
The IARC found that between 16-52% of women in the world were using talcum powder to dust their genitals and found that among them there was an increased risk of ovarian cancer ranging from 30-60%.
The Canadian government classified talc as a “D2A – Very Toxic” cancer-causing substance under its Hazardous Products Act. Notably, asbestos is similarly labeled as D2A.
The journal “Epidemiology” published the article “The Association Between Talc Use and Ovarian Cancer” in May 2016 which examined the association in 2,041 cases of ovarian cancer and genital talcum powder use. The article concluded with the observation that the use of talcum on the genitals is associated with elevated ovarian cancer risk vs. no increased risk among women who did not use talcum powder on the genitals.
A study headed up by Joellen M. Schildkraut, Ph.D., MPH, was published in the October 2016 journal “Cancer and Epidemiology, Biomarkers, Prevention”, which indicated that African American women had a substantially higher risk for ovarian cancer if they used talcum to powder their genitalia.
Regulators and the Industry
Manufacturers of talcum powder products are not required to provide safety information in the United States. The U.S. Food and Drug Administration (FDA) has opined in the past that it does not believe it has the authority to require any sort of warning on talcum powder. However, in 2016, the FDA’s Office of Women’s Health (OWH) did announce its funding of additional research into the potential for a relationship between talcum powder and ovarian cancer, acknowledging that its effects on female genitalia have not been adequately investigated. The OWH research is aimed at filling in “data gaps” in the association of talcum powder and the onset of cancerous conditions.
Johnson & Johnson and other talcum-based product manufacturers uniformly continue to insist that their products are both asbestos-free and do not cause cancer. In May 2020, Johnson & Johnson announced that it would discontinue sales of baby powder in North America.
2) “Estate of Maureen Broderick Milliken, Deceased v. Johnson & Johnson, et al.” Case 2:16-cv-02866-MAK, U.S. District Court, Eastern District of Pennsylvania.
Deep Vein Thrombosis (DVT) or blood clots that form in the large veins of the lower extremities sometimes progress to the point where they cause swelling, tenderness, and pain in patients. When DVTs break loose and travel through the body on the way back to the heart they become a potentially life-threatening risk in the form of a Pulmonary Embolism (PE). The frontline treatment for DVT is usually a prescription blood-thinner on either a temporary or permanent basis. However, where blood thinners are not an option, doctors may recommend the placement of an Inferior Vena Cava (IVC) filter as a solution.
As with any surgical procedure, implantation with an IVC filter presents a number of risks and benefits to patients. It is important that patients discuss the facts about IVC filters with their physicians and learn as much as possible about the risks and potential complications from these devices. Below are some of the more commonly asked questions about IVC filters which can form the basis for a broader conversation with your physician about DVT treatments and a comprehensive IVC filter strategy.
What is an Inferior Vena Cava (IVC) Filter?
IVC filters are small mechanical devices that surgeons place into the vein in order to prevent DVT and other types of blood clots from using the IVC as a highway back to the heart and lungs. They are spindly devices that look and act like a sifter – allowing clear blood components to pass through it while intercepting and catching clots.
Which Patients Typically Receive IVC Filters?
IVC filters are generally recommended for patients who suffer from chronic DVT and who cannot take blood-thinning medication. Sometimes, an IVC filter will be recommended to patients who are about to undergo surgery and have to suspend taking blood thinners temporarily.
Is an IVC Filter Implanted Permanently?
There are two general types of IVC filters on the market in the United States: permanent and optional (also known as “retrievable”). Permanent filters have been utilized in patients since the 1970s and are placed in patients with long-term needs to filter against PE or other issues with blood clotting. Retrievable filters are newer and as the name suggests, are designed to be retrieved from the patient (or sometimes left in place) after a temporary risk of PE or clotting has passed or been resolved.
How are IVC Filters Implanted?
The procedure for implanting an IVC filter typically involves a smaller incision made by an implanting physician in either the groin or neck. The doctor will then insert a flexible tube or “catheter” with a collapsed filter into a vein and route into the Inferior Vena Cava. Once it reaches the IVC, the filter is then triggered to expand and attach itself to the walls of the vein. In some cases, the filter becomes a permanent fixture in the IVC, although others are implanted with the understanding they will be removed after some period of time.
How Should I Prepare for IVC Insertion Procedure?
Prior to the procedure, your physician will likely order a series of blood tests to examine kidney function and blood clotting patterns. You should be very open and tell your physician about all medications – as well as herbal supplements that you take on a regular basis. Also, ensure that your physician is well aware of any recent illnesses or other medical conditions. Your physician will advise you as to which medications you can take either in advance or the day of the procedure as well as whether or not to eat or drink anything after midnight beforehand.
What is the Procedure Like?
IVC insertion is usually performed on an outpatient basis either in an operating room or in an interventional radiology suite. Patients are typically positioned on their back and are connected to a heart monitor. Usually, the procedure does not require general anesthesia and patients can be administered a solution intravenously which induces a sedated state. The physician will numb the insertion site and make a very small incision for catheter insertion. When the procedure is finished, the catheter is removed and pressure is applied to stop bleeding. Stitches are not usually required and a small dressing is applied to the small incision.
When Can Patients Go Home After the IVC Filter Insertion?
The insertion procedure is usually completed within an hour. Patients will remain at the medical center for up to 3-4 hours and then can return home. In some cases, your physician will order you to remain overnight at the hospital for observation.
What Should You Do When You Get Home?
Patients should avoid strenuous activities for at least a day or two. They can resume a normal diet and should consume fluids to avoid dehydration. A bandage should be kept over the incision site for at least a day or as long as your physician recommends. An ice pack can be placed on the site for 10-20 minutes at a time to help alleviate soreness and swelling.
What About Medications?
You should speak at length with your physician about all medications and supplements you are taking. She will let you know when to stop and restart any medication consistent with the procedure. Be safe with your medications and take them precisely as directed by your physician. If you think your medication is making you sick, advise your doctor immediately and discuss options for possible substitution.
Can Things Go Wrong with IVC Filters?
IVC filters have enjoyed widespread adoption and use – in particular following the introduction of optional or retrievable filters in the 1990s. However, with the increased use of the filter, has come a growing recognition that there are a number of safety complications associated with these devices. Some risks and complications associated with IVC filters include:
IVC Filter Fracture
IVC Filter Penetration
IVC Filter Migration
Excessive Tilting
Patients should have a frank and open discussion with their physicians about the type of device with which they are going to be implanted as well as the risks associated with that particular device.
If I Have a Removable Filter – When Should It Be Removed?
The U.S. Food and Drug Administration (FDA) has issued a recommendation concerning removable IVC filters. Specifically, the FDA believes that removable filters should be removed as soon as the risk of PE has subsided. Guidelines further state that removal should take place within 29-54 days following insertion (if possible).
The Inferior Vena Cava (IVC) is the largest vein in the human body and is located toward the anterior of the abdomen to the right of the aorta. The IVC has one function – to carry copious amounts of deoxygenated blood back from the lower extremities of the body and back to the heart. It is an essential part of human anatomy and is a central component of the human cardiopulmonary system.
Alongside the important role that it plays in maintaining life, the IVC can also develop issues that threaten life as well. Veins like the IVC can develop clumps of thickened blood which form clots. When clots form below the heart, and in particular in the thigh or lower leg, they are referred to as “Deep Vein Thrombosis” (DVT). If a DVT clot breaks free and makes its way back to the heart or lungs, it can become a deadly “Pulmonary Embolism” (PE). Once lodged in the chest cavity, a PE can block the flow of blood to the heart and lungs, significantly disrupting cardiopulmonary function.
Symptoms of Pulmonary Embolism
Symptoms of PE can vary dramatically from patient to patient. The size of the clot and its location in the lungs, as well as the underlying heart condition of the patient, can all play a large impact on the magnitude and duration of symptoms. Common signs of PE include:
Shortness of Breath
Chest Pain
Coughing
Rapid or Irregular Heartbeat
Lightheadedness or Dizziness
Excessive Sweating
Fever
Leg Pain or Swelling
Clammy or Discolored Skin
PE can be life-threatening. If you experience unexplained shortness of breath, chest pain, or a cough that produces bloody fluid – you should seek immediate medical attention.
Inferior Vena Cava Filters
IVC filters are small mechanical devices that surgeons place into the vein in order to prevent DVT and other types of blood clots from using the IVC as a highway back to the heart and lungs. They are spindly devices that look and act like a sifter – allowing clear blood components to pass through it while intercepting and catching clots.
IVC filters are generally recommended for patients who suffer from chronic DVT and who cannot take blood-thinning medication. Sometimes, an IVC filter will be recommended to patients who are about to undergo surgery and have to suspend taking blood thinners temporarily.
To implant an IVC filter, a physician or surgeon will make a small incision in either the groin or neck and then position the filter using a small catheter maneuvered through the incision. Once in place, the filter is “triggered” to expand and attach itself to the walls of the vein. Some IVF filters are permanently left in the vein while others are implanted with the understanding they will be removed later.
Issues with IVC Filters
IVC filters are not necessarily “new” technology. They were first cleared for use by the U.S. Food and Drug Administration (FDA) through the abbreviated 510(k) Clearance process in the late 1970s. However, their use expanded dramatically in a very short span of time between 1999 and 2008.
In 2010, the FDA, after noticing a spike of “adverse event reports” through the previous years, issued a warning about IVC filters and the potential for such issues as filter migration; embolization; perforation of the Vena Cava; and mechanical fracturing of the filter itself. The FDA’s warning was followed in 2014 with a “safety communication” concerning the filters and the agency instituted a new postmarket surveillance study to evaluate the growing use of IVC filters and to make additional recommendations.
IVC Filters and Migration
Experts have grown concerned that too many retrievable (temporary) IVC filters have been implanted into patients – and then never removed. IVC filters which are inserted on a temporary basis, but then left for a longer duration in the body can begin to shift inside of the vein. This is known as IVC filter migration – and it is a serious problem. There are three main types of IVC filter migration:
Mechanical: Typically, this involves the failure of the device itself. Surgeons will usually identify mechanical issues during surgical implantation.
Iatrogenic: Each IVC filter is measured and approved to fit specific measurements within the IVC itself. Iatrogenic migration occurs where the device doesn’t fit the placement properly due to guide wire entanglement.
Physiological: Bending, coughing, or straining while lifting could cause an IVC filter to dislodge and migrate.
Embolization (Migration into Heart and Lungs)
If the IVC filter migrates far enough away and into the functioning apparatus of the heart and lungs in the chest cavity, it can create life-threatening conditions that require urgent medical treatment.
Perforation of the Inferior Vena Cava
An implanted IVC filter is designed to attach and grapple onto the walls of the vein to remain in place. However, this same technique can sometimes also result in a tiny perforation of the vein causing damage to the IVC itself as well as to surrounding tissue and organs. Symptoms of a perforated IVC include:
Swelling
Pain
Pulmonary Embolism Symptoms (see above)
Some patients suffering from a perforated IVC also report progressively worsening abdominal or back pain over several weeks, later accompanied by bouts of nausea and vomiting. In any event, IVC implantees suffering from these symptoms should seek immediate medical attention and the care of a physician.
Filter Fracturing
When viewed in their operational position, IVC filters tend to resemble umbrellas in their design and function. Like an umbrella, the spindly legs which open inside of the vein are key to its function and to keep the filter in place. Some filters were designed to be implanted and stay in the body permanently. Others were designed to be implanted and then removed at a later date. Unfortunately, for patients with these “temporary” filters, the follow-up procedure to remove them is often forgotten or disregarded.
Temporary IVC filters that are left in the body can begin to degrade due to excessive wear and tear from the pressures exerted within the vascular system of the human body. Eventually, the spindly legs on the filter can break off or fracture – traveling through the body. Remember – all blood in the IVC travels toward the heart and lungs. Accordingly, a fractured filter can present a multitude of dire medical consequences for the patient including DVT, heart attacks, and internal bleeding.
The FDA and IVC Filters
To date, the FDA has yet to issue any formal recalls for any IVC filter device. Nonetheless, between 2005 and 2019, at least eight types of IVF filters have been voluntarily withdrawn from the market by their manufacturers. In its first warning letter concerning IVC filters in 2010, the FDA detailed over 921 injuries from IVC filters spanning: migration through the body; migration into the heart and lungs (embolization); perforation of the vena cava; and filter fracturing. Since 2014, filter manufacturers have been given the option of either participating in the FDA’s 522 Postmarket Surveillance Studies program or an independent clinical study known as “Predicting the Safety and Effectiveness of Inferior Vena Cava Filters” (PRESERVE).
Furthermore, filter manufacturer C.R. Bard was recently party to a now-settled case in multidistrict litigation over its filter products (MDL-2641). Cook Medical is currently a party to ongoing multidistrict litigation in federal court in Indiana (MDL-2570) over its IVC filter products.
Cook Medical is a business unit of the Cook Group Incorporated, a global privately-held conglomerate headquartered in Bloomington, Indiana. Established in 1963, the Cook Group is made up of five distinct business sub-units spanning: Hotels & Resorts; Property Management; Medical Services/Aviation and Component Manufacturing; Life Sciences; and Medical Devices. Today, the Cook Group employs more than 12,000 people around the world and last year reported revenue in excess of $2 billion. It is widely acknowledged to be one of America’s largest private companies.
The Cook Medical unit has attracted a great deal of attention on its own in recent years. Most recently the company made headlines for its Gunther Tip and Celect lines of Inferior Vena Cava (IVC) filter products which are the subject of multidistrict litigation currently underway before a federal court in Indiana. Claimants implanted with the Cook Medical IVC filters have alleged in court filings a number of serious injuries they believe were caused by manufacturing and design defects that Cook Medical allowed onto the market without adequate testing or refinement.
History and Background of Cook Medical
The story of Cook Medical began when company founder, Bill Cook, and his wife started making catheters in a spare bedroom of their apartment in Bloomington, Indiana, during the early 1960s. Aside from catheters, the duo also manufactured needles and wire guides. Despite its humble start, Cook Medical rapidly grew in sales and expanded internationally throughout the 1970s. By the 1990s, Cook Medical had diversified into intravascular coronary stents, programmable pumps, and infusion devices. Cook describes its approach to medical device manufacturing as “Minimally Invasive Medicine”.
Cook Medical’s IVC Filter Products
The Gunther Tulip
The Gunther Tulip is an IVC filter that has been marketed in the United States since 2003. It was designed as a retrievable filter, meaning it is only supposed to be implanted for short periods of time. If it is left in the vein for a long period of time (3-4 months), the Gunther Tulip increases in its risk of fracture or migration, which can lead to Pulmonary Embolism (PE) and possibly death.
Celect IVC
Similar in shape and design to the Gunther Tulip, the Celect line of IVC filter is a retrievable, umbrella-shaped filter made of a cobalt-chromium alloy. The Celect was approved through the 510(k) Clearance process (like the Gunther Tulip). And similar to other IVC filters, the Celect has the potential for fracture and migration the longer it is left inside of the human body.
Issues with Cook Medical Technologies and Product Lines
In re: Cook Medical, Inc. IVC Filters (MDL-2570)
Lawsuits revolving around the Gunther Tulip and Celect lines of IVC filters manufactured by Cook Medical began to make their way into courtrooms around the country in 2013 and 2014. These cases were then consolidated into multidistrict litigation in Indiana. The implantees in this MDL complained of alleged design and manufacturing defects such as tilt, migration, and fracturing. Specifically, some claimants referenced a study published in Cardiovascular Interventional Radiology in 2012 which assessed that the Gunther Tulip and Celect lines failed at a rate of 100% up to 71 days following implant and caused some degree of perforation of the wall of the vena cava. The same study reported that tilt was witnessed in 40% of the Gunther Tulip and Celect filter lines.
The outcomes of the various bellwether trials in this MDL have been a mixed-bag:
In November 2017, a jury sided with Cook Medical and failed to find the company liable.
A second bellwether case was dismissed in April 2018 due to statute of limitation issues.
A Houston firefighter was awarded $1.2 million by a Texas jury in May 2018 (not actually a bellwether case and not part of the MDL).
In December 2018, the presiding judge in the MDL granted summary judgment to Cook Medical in a Georgia case brought by Tonya Brand.
Most recently, in February 2019, an Indiana jury awarded $3 million to a woman who suffered a range of injuries from one of its IVC filter lines.
While PPIs have proven very useful for the treatment of chronic maladies such as Gastroesophageal Reflux Disease (GERD), patients should be aware that they also have the potential to interact with certain other common medications. Accordingly, PPI users should consult with their physician about what other types of medication or supplements they take in order to reduce the possibility of adverse reactions.
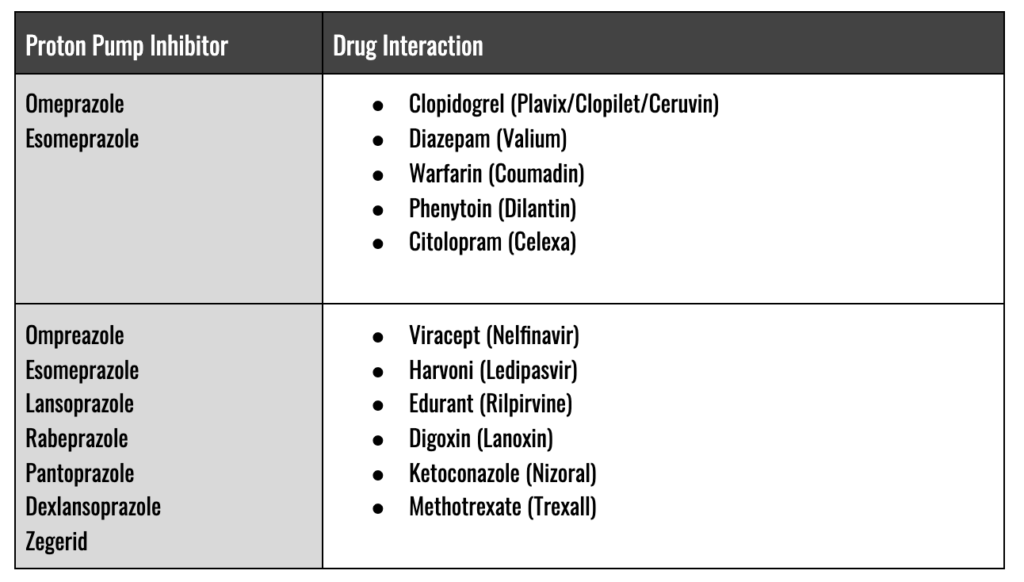
PPIs and Common Drug Interactions
Omeprazole, perhaps one of the most commonly prescribed and purchased PPIs on the market is believed to interact with at least 194 drugs on the market today. Of these interactions, at least 16 are believed to be serious, 132 are thought to be moderate and 46 are minor.
Omeprazole (Prilosec) and Esomeprazole (Nexium) Interaction with Clopidogrel
Clopidogrel (brand names: Ceruvin, Clopilet, and Plavix) is an anti-clotting medication that is commonly prescribed for patients suffering from heart disease or who are at increased risk for heart attack and stroke.
Clopidogrel’s effectiveness as an anti-clotting agent is frequently accompanied by one very common side effect: it causes significant disruption of the lining of the stomach and intestines. Sometimes this disruption can also increase the risk of gastrointestinal bleeding. Furthermore, doctors may also prescribe an aspirin regimen alongside clopidogrel, especially after placement of an arterial stent. Since clopidogrel and aspirin both have issues with excess stomach acid, physicians would commonly prescribe PPIs such as omeprazole and esomeprazole to patients to help ease this side effect.
Unfortunately, most PPIs, and in particular omeprazole and esomeprazole, stall the production of an enzyme known as “CYP2C19” that is critical to the body’s ability to metabolize clopidogrel. Consequently, the U.S. Food and Drug Administration (FDA) issued a warning in 2009 asking patients taking clopidogrel to avoid omeprazole and esomeprazole.
PPIs and Alcohol Consumption
Alcohol, in particular red wine and distilled spirits such as tequila, rum, and whiskey, are frequent culprits that trigger heartburn or other symptoms associated with GERD. The effect of alcohol on heartburn can be doubled or worse by combining alcohol with caffeine-boosted beverages.
People who suffer from heartburn or GERD frequently turn to OTC medications such as antacids, H2 blockers (Pepcid, Tagamet, Zantac, and Axid), and PPIs. Although there are no clear drug interactions between PPIs and alcohol use, it should be noted that the impact of PPIs can be lessened by excessive alcohol consumption. Furthermore, PPIs can mask other conditions such as gastric ulcers which can be exacerbated by excessive alcohol consumption.
Onglyza is the brand name of the well-known anti-diabetic medication saxagliptin. Kombiglyze XR is the brand name of another anti-diabetic drug that combines saxagliptin and metformin HCL into one medication. Both drugs are prescribed to help sufferers of Type 2 Diabetes Mellitus (T2DM) better manage blood sugar levels. They are meant to be used in conjunction with diet, exercise, and other medications as part of a larger treatment strategy combating T2DM.
Although Onglyza and Kombiglyze present a novel treatment option that offers hope to a range of T2DM sufferers, they also carry with them a list of possible undesirable side effects that vary from less serious to potentially life-altering. According to the U.S. Food and Drug Administration (FDA) and the manufacturers of Onglyza and Kombiglyze, the following are some of the side effects noted during development and testing:
Sore Throat
Headache
Joint Pain
Rash
Hives
Skin Peeling
Itching
Swelling of the Face, Lips, Tongue, or Throat
Difficulty Breathing or Swallowing
Hoarseness
Vomiting
Loss of Appetite
Excessive Tiredness
Shortness of Breath
Swelling of the Feet, Ankles, or Legs
Sudden Weight Gain
Risk of Heart Failure
In 2015, researchers and physicians collected information as part of a comprehensive effort to study any potential association between saxagliptin and increased risk for heart failure. The study, known as “Saxagliptin Assessment of Vascular Outcomes Recorded in Patients with Diabetes Mellitus” (SAVOR), found that saxagliptin may increase the risk of hospitalization for heart failure by about 27%.
These results, in combination with other research findings, prompted the FDA to convene an advisory panel in April 2015 which concluded that saxagliptin may indeed increase the risk of heart failure in individuals taking the medication. On the heels of the advisory panel recommendations, the FDA issued a Drug Safety Communication in April 2016 warning of the increased risk. These warnings were also added to the drug labels for Onglyza and Kombiglyze.
To put the risk into perspective, the SAVOR trial examined patients taking saxagliptin for two years and noted the following:
3.5% of patients taking Onglyza were hospitalized for heart failure, compared to 2.8% for those who received a placebo. Put another way – if 1,000 people suffering from T2DM took Onglyza, 35 of them may theoretically be hospitalized for heart failure as opposed to 28 sufferers not taking the drug.
Overall, those taking Onglyza had no increased risk of heart attack, stroke, or death from heart disease than those on placebo during the study.
People with preexisting heart disease history or kidney disease would have an increased risk of heart failure on Onglyza. The FDA recommends that prescribing physicians consider discontinuing the use of saxagliptin in patients who develop heart failure during treatment.
Pancreatitis and Pancreatic Cancer Risk
The British Medical Journal (BMJ) published an article in 2013 which shed light on growing safety concerns surrounding incretin mimetics. The article suggested that risks for developing pancreatitis and pancreatic cancer associated with these drugs were being downplayed. However, a follow-up investigation by the National Institute of Diabetes, Digestive and Kidney Diseases (NIDDIK) suggested that there was likely no increased risk of either ailment associated with incretin mimetics.
The FDA has issued a public warning about pancreatitis and pancreatic cancer associations with incretin mimetics. Furthermore, the agency announced that it would investigate ongoing post-market reports concerning pancreatic ailments, including pancreatic duct metaplasia in patients.
Joint Pain
In August 2015, the FDA issued a warning statement that saxagliptin may cause severe and disabling joint pain in patients. The warning followed an analysis of reports within the FDA’s own Adverse Event Reporting System (FAERS) database which noted that patients started having symptoms from one day to years after starting to take saxagliptin. After the patients stopped taking saxagliptin, their symptoms were relieved and tended to restart if they went back on the medication.
The FDA warning noted that patients should not stop taking saxagliptin but should contact their physician right away if they experience severe and persistent joint pain. Furthermore, health care professionals should consider saxagliptin (and similar drugs) as a possible cause of joint pain and discontinue the drug if appropriate.
Metallosis is a condition where human tissue and bodily systems are damaged/degraded by contamination from metallic corrosion and the release of toxic metallic debris into the bloodstream. Tissue impacted by metallic corrosion and leaching suffer pain and appear discolored due to “Adverse Local Tissue Reaction” (ALTR) or “Adverse Reaction to Metal Debris” (ARMD).
Depending upon the nature of the metal-alloys present (and other factors), corrosion and leaching can develop into metallosis and more potentially painful joint symptoms as well as dermatologic conditions, depression, dementia, renal failure, cardiovascular issues, and pseudotumors.
Metallosis has been found to occur as a side effect of hip joints composed of the metallic femoral stem and head combinations – also known as “metal-on-metal” (MoM). In years past, titanium and stainless steel were prevalent in many lines of implantable hip joints. However, in recent years cobalt-chromium combinations emerged as the most desirable for metal-on-metal (MoM) hip implants.
Metal-on-Metal Hip Implants
Beginning in the early 2000s, manufacturers like DePuy, Zimmer, Stryker, and Smith & Nephew all aggressively brought MoM hip joint lines to market through the U.S. Food and Drug Administration’s (FDA) abbreviated 510(k) clearance process. This “fast-track” review allowed manufacturers to bring new MoM hip joints to the market rapidly without having to engage in clinical trials or extensive testing.
MoM hip implants are characterized by a metallic ball and cup pairing which slide against each other when the joint functions (i.e. activities such as walking or running). When the two metal couplings rub each other, metal can begin to shed from the device causing particles to embed in surrounding tissue as well as metallic ions to enter the bloodstream and disperse throughout the body. These particles and ions can progress to metallosis.
As far back as the 1970s, surgeons have recognized the heightened association between MoM and metallosis. Dr. George McKee, a surgeon in the United Kingdom, first reported metallosis in patients who developed painful symptoms 3-4 years following hip replacement with a MoM joint. Dr. McKee’s patients reported progressive pain and instability and upon examination, showed soft tissue that appeared stained green with a grey paste accompanied by bone loss. Large amounts of joint fluid were also reported – either rust, green, cloudy yellow, or grey-colored in appearance.
In May 2016, the FDA shifted its approach to MoM hip joints, requiring all manufacturers to immediately cease and desist from marketing MoM devices until their safety and efficacy could be demonstrably proven with valid supporting scientific evidence. Since that time, no MOM hip replacement devices have been approved for the market in the United States.
Cobalt-Chromium Hip Implants
Cobalt chromium was first used for hip arthroplasty in 1938 by Dr. Marion Smith-Peterson. Dr. Smith-Peterson found that the cobalt-chromium alloy was preferable to others due to its relatively inert nature. As a general rule, any metal alloy implanted into the human body will undergo ionization and start the process of corrosion. However, cobalt-chromium showed itself to be more corrosion-resistant than others.
The same wear and tear associated with other MoM devices can also be a source of cobalt poisoning or acute cobalt toxicity. In addition to other symptoms associated with metallosis, cobalt toxicity can also cause patients to suffer from fevers, inflammation, low thyroid levels, loss of hearing and vision, organ damage, and even heart failure.
Symptoms of Metallosis
Metallosis symptoms typically do not emerge right after hip replacement. They emerge gradually over time. In some cases, metallosis has been reported to manifest anywhere from 3-4 years following surgery. Generally, the symptoms associated with metallosis include:
Pain around the implant joint
Pseudo-tumors (nodules resembling tumors – but which are actually fluid collecting)
Rash
Osteolysis
Loosening of the joint
Raised levels of cobalt and chromium in the blood.
Metallosis and Depression/Dementia
In a 2017 article for BMC Psychiatry, Dr. Ben Green, Dr. Emily Griffiths, and Dr. Solomon Almond examined ten pre-revision surgery patients, nine of whom were suffering from toxic levels of chromium and cobalt in their blood. Among the nine patients, all reported significant levels of depression. Seven of the ten patients had neurocognitive abnormalities, including short-term memory deficits, problems with concentration, and difficulties verbalizing.
Metallosis Treatment Options
Generally speaking, the only option for MoM hip implant patients suffering from complications from metallosis is revision surgery. During revision surgery, the physician will work to excise affected bone and soft tissue around the joint. For more severe cases of metallosis, a surgeon may also elect to resurface. In all cases, the new joint implanted will feature a new stem, head, and acetabular combo likely with either a ceramic or plastic component. The good news for patients is that once the revision is complete, they usually recover quickly.
Generally, hip placement surgery – also known as Total Hip Arthroplasty (THA) enjoys a favorable rate of success in patients. However, even under the best of circumstances, THA can still fail for any number of reasons. If a hip replacement procedure is unsuccessful or does not otherwise meet expectations, a surgeon may recommend a follow-up procedure to either remove or replace some or all of the implanted device. This type of surgery is known as a “revision”
Reasons for Hip Revision Surgery
Patients who undergo THA can usually expect that their prosthesis will last at least 15-20 years – and in some cases, remain within the patient for the rest of their life. However, in approximately 18% of all hip replacement scenarios, doctors will recommend revision surgery. The most typical factors mitigating in favor of revision are:
Recurrent or Repetitive Dislocation of the Hip Joint
Traumatic hip dislocation can occur where the ball of the hip joint is pushed out of the socket. A dislocated hip can be debilitating if not addressed to put the ball and socket back into proper alignment and ensure proper complementation by surrounding muscle and ligament tissue.
Fortunately, dislocation is a relatively infrequent phenomenon among younger patients who follow proper care guidelines given by their physician. However, among elderly patients or those who have THA following fracture, rates of dislocation rise precipitously. Furthermore, patients who have already suffered dislocation are more likely to suffer additional dislocations without corrective surgery as surrounding tissue becomes increasingly disrupted.
Infection
Infection resulting from any surgical setting, including hip replacement, is a very real problem and a possibility all patients must face. Exposure to infectious bacterial agents can occur even in surgical theaters observing even the most stringent sterilization protocols. Additionally, patients who suffer from conditions such as diabetes mellitus, obesity, peripheral vascular disease, or are immunocompromised, may be at even greater than usual risk for infection.
The risk for infection is greatest within the first six weeks following surgery. If infection sets into the prosthesis, the surgeon will usually recommend a battery of tests to identify the type of infectious agent at work, possibly including an aspiration of joint fluid from the hip joint itself.
Once the surgical team identifies the type of infection, they will consider a range of treatment options. Chief among these is the use of targeted antibiotics and revision surgery to eradicate the infection. Typically revision procedures to address infection include:
Surgical cleansing with intravenous antibiotics.
A complete exchange of the hip replacement device:
Two-Stage:The surgeon will remove the device and infection then clean the bone. A temporary cement spacer will be implanted while the patient undergoes a six-week course of intravenous antibiotics. Following the antibiotic treatment, a new prosthetic device will be implanted.
Single Stage: This procedure entails the removal of the device, total cleansing of the infected joint, and replacement with a new device all at once. Like the two-stage procedure, patients will require six-to-eight weeks of intravenous antibiotics afterward.
Wear and Tear/Loosening
The metal, ceramic and plastic components of a hip joint replacement will rub against each other as part of the normal function of the prosthesis. Over time, however, joint movement can slowly wear down parts of the implant increasing the risk of failure or revision.
Excessive vigorous physical activity by younger/more active patients
Obesity
The type of device (i.e. “metal on metal” vs. “metal on polyethylene” vs “metal on ceramic”)
In some cases, wear and tear from the device will introduce synthetic particles into surrounding tissue as well as the patient’s bloodstream. These particles can then trigger an immune response that fosters progressively worse conditions such as osteolysis (destruction of surrounding bone tissue).
In Metal-on-Metal (MoM) hip implants, the metal ball and metal cup slide against each other during walking or running. This friction between the ball and socket can cause the release of metal particles which will wear off of the device and embed in surrounding tissue as well as metal ions of cobalt and chromium entering the bloodstream. Over time, this leaching of metal from the joint into surrounding tissue causes “Adverse Local Tissue Reaction” (ALTR) and/or “Adverse Reaction to Metal Debris” (ARMD). The bottom line for patients implanted with MoM joints, however, is that they suffer damage and pain, device failure, loosening, and the need for revision surgery. Furthermore, patients implanted with MoM hip joints can also suffer from a condition known as “metallosis” – a potentially fatal complication arising from metallic erosion in the joint which induces pain around the joint, pseudotumors, and a noticeable rash.
What to Expect with Hip Revision Surgery
Pre-Operative Protocols
In the weeks and days prior to revision surgery, doctors will order a variety of tests such as X-rays, CT and bone scans to identify the issues which they seek to address during the procedure. Additionally, they may ask for a routine aspiration of the joint to rule out infection risks prior to surgery. Patients should make arrangements for post-surgical assistance around the home and consult with their personal physician concerning medications or other relevant physical conditions. It is recommended that patients stop smoking as long as possible before surgery.
The Revision Procedure
A hip revision can be a longer and more complex procedure than the original THA surgery. A simple revision can just be a swap of liner components. A more complex revision can be as involved as a total replacement of all components. However, effective planning and coordination between the surgical team and your personal physician can help ward off more serious complications during and after the revision procedure.
Post-Operative Matters
Following revision surgery, patients may be allowed to sit up out of bed or even walk the very next day upon the advice of their surgeon. Some pain, but not excessive pain, is to be expected. Patients are typically discharged to their home or to a rehabilitation hospital within 5-7 days post-revision. Afterward, they will usually transition into a physical therapy regimen accompanied by the use of crutches and canes for walking assistance for as many as six weeks.
Complications and Risks from Revision Surgery
Revision surgery, like other major procedures, is not without inherent risk. Possible medical complications associated with any surgery include, but are not limited to:
Allergic Reactions to Certain Medications
Blood Loss
Heart Attacks/Strokes/Kidney Failure/Pneumonia
Nerve Damage
Risks more commonly associated with THA and revision surgery also include:
Deep Vein Thrombosis (DVT) is a widely recognized risk factor following hip revision surgery. DVT is a blood clot in the leg that can break loose and become a Pulmonary Embolism (PE) that travels through the body and into the lungs where it can cause illness and death. DVT can occur in any vein in the body, however, they tend to manifest the most often in the lower extremities of the body.
Infection following revision surgery is a possibility and a very serious problem. Accidental exposure to bacteria such as staphylococcus aureus can occur even in the midst of the most stringent sterilization protocols. Common postoperative infection symptoms include swelling, stiffness, pain, redness, fevers, night sweats, and chills.
Metal-on-Metal Hip Implants and Higher Rates of Revision Surgery
Starting in the early 2000s, several manufacturers aggressively marketed hip-joints through the 510(k) process featuring a “Metal-on-Metal” (MoM) coupling feature between the ball and socket of the joint. In MoM joints, the metal ball and metal cup slide against each other during walking or running. This friction between the ball and socket can cause the release of metal particles which will wear off of the device and embed in surrounding tissue as well as metal ions of cobalt and chromium entering the bloodstream.
The bottom line for patients implanted with MoM joints is that they suffer damage and pain, device failure, loosening, and the increased need for revision surgery. Furthermore, patients implanted with MoM hip joints can also suffer from a condition known as “metallosis” – a potentially fatal complication arising from metallic erosion in the joint which induces pain around the joint, pseudotumors, and a noticeable rash.
Recalls and Lawsuits of MoM Hip Replacement Devices
Smith & Nephew Metal-on-Metal and Hip Resurfacing
Smith & Nephew is a United Kingdom-based joint device manufacturer with operations in the United States. In 2017, Smith & Nephew was named a defendant in Multidistrict Litigation (MDL-2775) occurring in federal court in Maryland before Judge Catherine C. Blake. At the center of the litigation naming Smith & Nephew are several hundred claims alleging defects involving the company’s MoM Birmingham Hip Resurfacing (BHR) implants and its R3 hip joint products. The BHR was the subject of a recall for all units implanted between 2006 and 2015 due to high rates of failure and revision surgeries as was the R3 in 2012 due to issues with erosion and metallosis.
Stryker LFIT V40 Femoral Head and Rejuvenate/ABG II Hip Implant
Stryker is a Michigan-based medical device manufacturer that traces its founding back to Dr. Homer Stryker, an orthopedic surgeon, and his device inventions dating back to 1941. Today Stryker is an international giant that claims $14.9 billion in sales in 2019. In 2016, Stryker announced a recall of its LFIT V40 femoral heads manufactured before 2011 following post-market surveillance showing a higher-than-average rate of failure with symptoms in patients similar to those suffering from metallosis. Similarly, Stryker recalled its Rejuvenate and ABG II implants in 2012 (after only 2 years on the market due to post-market research indicating issues common to MoM devices. Both the LFIT V40 and the Rejuvenate/ABG II devices are the subject of ongoing multi-district litigation in federal court in Massachusetts (MDL-2768) and Minnesota (MDL-2441).
DePuy Orthopedics ASR Hip Implant and Pinnacle Hip Implant
DePuy Synthes is a subsidiary of global pharmaceutical and medical device manufacturer Johnson & Johnson. In 2010, DePuy Synthes issued a voluntary global recall for its ASR Acetabular System following evidence that emerged through post-market surveillance that patients were suffering considerable pain, immune system reactions, inflammation, and the need for revision. The symptoms were consistent with MoM injury and potential design flaws. Similarly, Depuy Synthes’ Pinnacle MoM hip implant is alleged to cause a condition called “osteolysis” which occurs when bone surrounding the hip joint dissolves due to instability and metallosis. Pinnacle has not been the subject of a recall as of this date. However, both the ASR Hip Implant and the Pinnacle Hip Implant are subjects of multi-district litigation in Ohio (MDL-2197) and Texas (MDL-2244).
Zimmer M/L Taper Hip Prosthesis and Versys Femoral Head (MDL-2859)
Indiana-based Zimmer Biomet Holdings, Inc. developed and marketed the Zimmer M/L Taper hip implant with its proprietary Kinectiv Technology. This model of the M/L Taper with the Kinectiv technology utilized a modular MoM design that featured a cobalt-chromium coupling. In court documents, claimants allege that the Zimmer hip joint suffers from corrosion which introduces metal fragments into surrounding tissue as well as elevated levels of metals into the bloodstream causing pain, swelling, tissue necrosis, and other ailments.
A hernia is a condition where an organ, intestine, or fatty tissue (typically in the abdomen) pushes through a weak spot in a surrounding muscle or connective tissue. They are usually caused by a combination of pressure and the development of the weak spot. Hernias are more common later in life – although they can manifest at birth. Factors contributing toward hernia development are obesity; lifting heavy objects; diarrhea or constipation; or persistent coughing/sneezing. Additionally, poor nutrition, smoking, and overexertion can contribute to the formation of a hernia.
The only way to repair a hernia is with surgery. Hernia surgery is one of the most common surgical procedures performed worldwide. The most straightforward method is for a surgeon to make an open incision into the abdomen and then attempt to repair the breach in the tissue wall with sutures. However, this type of procedure has a high rate of “recurrence” meaning that the sutures do not hold up well over time and further procedures become necessary.
As an alternative to sutures, surgeons prefer to use mesh devices as a tool to strengthen the area around hernias and make a repair that has less possibility of recurrence. Historically, surgical mesh has been used to repair hernias for well over a century in the United States. Today, more than 80% of hernia repair procedures performed in the U.S. involve mesh and there are more than 70 types of mesh commercially available.
Hernia Surgical Mesh Treatment Options
The most common type of hernia repairs involve inguinal hernias. Other types of repair procedures can involve the following types of hernias:
Femoral
Inciscional
Ventral
Umbilical
Hiatal
For some types of hernias, surgeons may elect to take a “wait-and-see” approach if the patient is not experiencing any serious complications. Instead, they will opt, with the patient, to monitor the hernia to ensure it is not getting any larger or causing other issues.
When surgery is a necessity, doctors will opt for one of two incision protocols based upon the patient’s condition and needs. The choice of the incision will also inform their choice of mesh device.
Laparoscopic: This involves the surgeon making a small incision in the abdomen which will allow for surgical tools to be inserted to effect hernia repair. Not all mesh devices are well-suited for this type of procedure.
Open Repair Surgery: This is a more traditional incision near the hernia for the purpose of repairing weak muscle tissue. If sutures are used instead of mesh, the procedure is referred to as a “primary closure”
Among laparoscopic incisional procedures, surgeons will choose a repair “approach” to effectuate repair. The most common approaches involve the position of the hernia relative to the peritoneum – the tissue lining your abdominal wall. Accordingly, these approaches are referenced as:
Transabdominal Preperitoneal (TAPP): The surgeon will go into the peritoneal cavity to place a mesh device over possible hernia sites.
Totally Extraperitoneal (TEP): The surgeon will not enter the peritoneal cavity and mesh will be used to seal a hernia from outside of the peritoneum.
Intraperitoneal Onlay Mesh Technique (IPOM): Introduced in the early 1990s, IPOM involves a small incision where gas is blown into the abdomen to get better visibility for the surgeon. Once surgical tools are inserted through the incision, surgeons can place and suture a hernia mesh directly onto the peritoneum where it can come into contact with the intestines or other abdominal organs.
Types of Hernia Mesh
Surgical hernia mesh is typically constructed either from animal tissue or entirely man-made (“synthetic”) materials. Synthetic mesh, such as those made from polypropylene, are made into “knitted” or “non-knitted” sheet formats. Furthermore, they can be “absorbable” or “non-absorbable” materials – or even a combination of the two. The animal-derived mesh is usually considered to be absorbable and will degrade over time while promoting new tissue growth to strengthen the hernia repair. Consequently, the absorbable mesh is not generally regarded as a long-term repair solution.
Potential Issues and Complications with Hernia Mesh
Most new mesh brands, in particular the synthetic ones, were “fast-tracked” for review by the U.S. Food and Drug Administration (FDA) through its abbreviated 510(k) clearance process which does not require stringent testing or clinical trials prior to implantation. In post-market surveillance, some common mesh brands have been associated with the following issues in patients:
Migration: Movement of the hernia mesh within the body.
Contraction: The mesh will collapse on itself and no longer cover the hernia location.
Adhesion: Scar-like tissue creation that can cause the tissue to “stick” or bind together.
Fistula: Leakage into body cavities or through the skin due to an abnormal connection between the organs or intestines.
Perforation: A hole or the bowels or neighboring organs due to contact irritation or an abrasion from the mesh.
Some mesh devices have been the subject of recalls and litigation. If you were implanted with a hernia mesh product and you are now experiencing pain and/or having to undergo invasive revision or removal surgery, you may be interested to explore your options for receiving compensation for suffering and medical expenses.
7) “The clinical effectiveness and cost-effectiveness of open mesh repairs in adults presenting with a clinically diagnosed primary unilateral inguinal hernia who are operated in an elective setting: systematic review and economic evaluation.” https://www.ncbi.nlm.nih.gov/books/NBK326920/
Drug Law Journal's publishing and research are sponsored by the DDP Injury Law Group in Washington, D.C. Their legal team is focused on protecting the rights of injury victims. Furthermore, they understand and appreciate the importance of a trusted attorney-client relationship. The DDP Injury Law Group uses their years of experience with litigation to ensure their clients can fight for the compensation they deserve.
Always seek the advice of a medical professional when making personal health choices.
The Offices of DrugLawJournal.com are located at:
1800 North Orange Avenue, Suite C
Orlando, Florida 32804
DrugLawJournal.com is sponsored by the DDP Injury Law Group, and therefore may be considered attorney advertising. The information contained on DrugLawJournal.com is provided for informational purposes only, and should not be construed as legal or medical advice on any subject matter. No viewers of this site should discontinue taking a prescribed medication on the basis of any information on this site and should always first consult with a doctor concerning any medication. Viewers should understand that if they refrain from taking prescribed medication without appropriate medical advice they can suffer injury or death.
No viewers of content from this site, clients or otherwise, should act or refrain from acting on the basis of any content included in the site without seeking the appropriate legal or other professional advice on the particular facts and circumstances at issue from an attorney licensed in the viewer’s state. Viewing information from DrugLawJournal.com does not create an attorney-client relationship between you and DDP Injury Law Group or DrugLawJournal.com nor is it intended to do so.The content of DrugLawJournal.com may not reflect current legal developments, verdicts or settlements. Prior results do not predict a similar outcome. For more information, please visit our web site’s disclaimer.
Sign up to receive peroidic updates from our expert team of researchers, highlighting defective drugs, devices, and legal issues related to your health.
It is important for those who have suffered injury from dangerous drugs and medical devices to know that they have may have options.
Consumers have the ability to seek legal remedies for their injuries resulting from the negligence of drug and device manufacturers. The first step toward justice and recovery is sharing your story with effective legal counsel. An attorney will help you to better understand the issues and discuss the possibility of compensation for your suffering.
Once you complete the information request above, Drug Law Journal will send the information to a specialist at our legal sponsor’s firm, the DDP Injury Law Group, in Washington, D.C. That specialist will follow-up with you directly to gather further specific information about your case and make an evaluation. If the firm is able to move forward on your case, they will also discuss next steps. Remember – the entire consult and evaluation is free to you. You only need to take the first step to fill out the contact form or call: (800) 597-1870 for immediate assistance.